Knee pain is one of the most common complaints of Americans of all ages. The pain can result from an injury, arthritis or other condition. The location and severity of knee pain often varies with each person depending on the cause of the problem.
Signs and symptoms of knee pain include: Swelling Redness Stiffness Weakness or instability Popping or crunching noises Inability to fully straighten the knee The pain in your knee can be caused by a number of factors.
Common causes of knee pain are: Injury A knee injury can affect any of the many ligaments, tendons, cartilage or bursae sacs that surround or consist of the knee joint.
Some of the most common knee injuries are: Anterior cruciate ligament (ACL) Meniscus Bursitis Tendinitis
It may start with an occasional twinge in your hip or a catch in your knee. Then you notice that actions you took for granted — climbing stairs, going for a long walk or squatting down to pick up a grandchild — take that twinge to an ongoing ache. Before you know it, you’re avoiding those activities.
More than likely, the culprit is osteoarthritis. This is the most common form of arthritis, and typically the result of wear and tear on your joints. It also may be caused by an old injury that 20 or 30 years later has come back to haunt you. For some people, it runs in the family.
Osteoarthritis is the loss of the smooth coating on the end of your bones called cartilage. Cartilage allows your joints to move easily and without pain. As the cartilage thins, the bones start rubbing together, causing inflammation and pain.
Here are 5 things you need to know about finding relief:
Maintain a healthy weight. Excess weight puts greater strain and pressure on your joints. Even modest decreases in your weight can make a big difference in the pain you experience.
Stay active. When it comes to joints, motion is the lotion to keep them working smoothly. Rather than jogging or playing tennis, choose low-impact activities like biking, walking and swimming. Pool exercise is a great option, providing buoyancy that takes strain off your joints; resistance of the water builds strength.
Limited access to healthcare Many rural residents live long distances from hospitals or specialty clinics, making it difficult to access regular care, schedule follow-up visits, or obtain prescription refills.
In addition, rural areas often suffer from a shortage of healthcare providers, especially pulmonologists who are essential for early diagnosis and disease management. This disparity is often due to rural regions receiving less healthcare funding and fewer resources than urban areas.
COPD is often referred to as a “smoker’s disease” however although smoking is one of the main risk factors for developing COPD, people who never smoke may also develop COPD. Other risk factors may include:
A history of childhood respiratory infections Smoke exposure from coal or wood burning stove Exposure to secondhand smoke People with a history of asthma People who have underdeveloped lungs Those who are age 40 and older as lung function declines as you age While these causes and risk factors may increase your risk of developing COPD, people living in poverty and people living in rural areas are more likely to develop COPD. Beyond smoking status, some reasons for the increased risk of developing COPD may include exposures to indoor and outdoor pollutants, occupational exposures and lack of access to healthcare.
Chronic obstructive pulmonary disease (COPD) is a progressive lung condition that makes it difficult to breathe and can significantly impact quality of life.
While COPD affects people across all regions, research from the U.S. Centers for Disease Control and Prevention (CDC) recently found that COPD is more prevalent and often more severe in rural areas. The data from the CDC shows that:
The percentage of adults in rural areas with COPD was 8.2%, which is double that of adults with COPD in large metropolitan areas.
Hospitalizations for COPD among Medicare enrollees in rural areas were about 14 per 1,000, but only about 11 per 1,000 in large metropolitan centers.
Death rates from COPD in rural areas were about 55 people per 100,000, compared to 32 people per 100,000 in large metropolitan areas.
Khazenay Bakhsh, DO, a pulmonary disease expert at Loma Linda University Health, says that the disparity stems from a complex mix of lifestyle, healthcare, and economic factors that create unique challenges for rural populations.
Chronic obstructive pulmonary disease (COPD) is a common lung disease. Having COPD makes it hard to breathe.
There are two main forms of COPD:
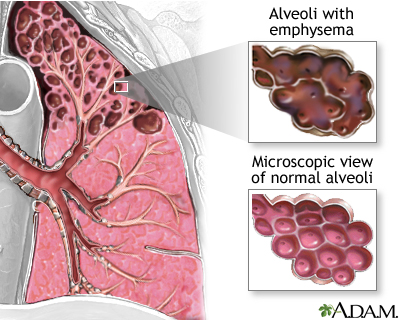
Chronic bronchitis, which involves a long-term cough with mucus Emphysema, which involves damage to the lungs over time Most people with COPD have a combination of both conditions.
Causes Smoking is the main cause of COPD. The more a person smokes, the more likely that person will develop COPD. But some people smoke for years and never get COPD.
If a person has a rare condition in which they lack a protein called alpha-1 antitrypsin, they can develop emphysema even without smoking.
As GPs, we see firsthand the toll that chronic obstructive pulmonary disease (COPD) takes on our patients.
It is a serious, progressive condition and remains one of the leading causes of death in Australia.
Early recognition and accurate diagnosis are vital in slowing disease progression, improving quality of life and reducing hospitalisations.
Yet we know that diagnosing COPD can be challenging in general practice.
Clinical features and chest X-rays alone are not enough; accurate diagnosis requires high-quality spirometry.
Despite this, access to and utilisation of spirometry can vary significantly, with implications for the quality of care patients receive.
To support GPs in this area, the Australian Commission on Safety and Quality in Health Care (ACSQHC) has introduced Practice Reflections: COPD.
This is a new quality improvement initiative designed specifically for GPs.
Each GP will receive a personalised, confidential report that uses their own MBS data to provide insights into how often office spirometry is being used compared to peers.
Importantly, this is not an audit or assessment.
The data is provided only to the recipient GP to support self-directed professional reflection.
Each GP will know how best to interpret the data, taking into account whether spirometry is performed at the practice, outsourced, or perhaps done while a patient is in hospital.
By comparing our own data with that of our peers, we can identify opportunities to align more closely with best practice COPD management guidelines, consider the barriers in our own context and reflect on what improvements might be achievable.
The first COPD Clinical Care Standard offers further guidance on what essential care for COPD should look like.
When used alongside the Practice Reflections report, it provides a valuable prompt for GPs to confirm diagnosis with spirometry, review patients managed without prior testing and ensure our care reflects the current evidence.
As clinicians, we all want the best outcomes for our patients.
This Practice Reflections report is an opportunity to pause, review and reflect on our role in diagnosing and managing COPD, and ultimately to support better patient care.
All qualifying GPs will automatically receive a printed Practice Reflections: COPD in November this year – learn more on the ACSQHC website.
Associate Professor Liz Marles is a GP and clinical director of the Australian Commission on Safety and Quality in Health Care.
COPD (chronic obstructive pulmonary disease) is a common progressive lung disorder characterised by airway obstruction with little or no reversibility. This irreversibility distinguishes it from asthma, in which airway obstruction is reversible. COPD is the third leading cause of death worldwide and accounted for 2.7% of all registered deaths in Hong Kong in 2017. Smokers are significantly more likely to develop COPD. Although there is no cure for COPD, it is treatable and preventable. Read more to learn about the causes, symptoms, prevention and treatment of COPD.
Chronic obstructive pulmonary disease (COPD) is a progressive lung condition that makes it difficult to breathe and can significantly impact quality of life.
While COPD affects people across all regions, research from the U.S. Centers for Disease Control and Prevention (CDC) recently found that COPD is more prevalent and often more severe in rural areas. The data from the CDC shows that:
The percentage of adults in rural areas with COPD was 8.2%, which is double that of adults with COPD in large metropolitan areas.
Hospitalizations for COPD among Medicare enrollees in rural areas were about 14 per 1,000, but only about 11 per 1,000 in large metropolitan centers.
Death rates from COPD in rural areas were about 55 people per 100,000, compared to 32 people per 100,000 in large metropolitan areas.
Khazenay Bakhsh, DO, a pulmonary disease expert at Loma Linda University Health, says that the disparity stems from a complex mix of lifestyle, healthcare, and economic factors that create unique challenges for rural populations.
A COPD flare-up, or acute exacerbation, is a worsening of your COPD symptoms. Flares may require hospitalization; they also can be life-threatening. According to the American Lung Association, most are caused by respiratory infections, such as a cold, the flu, COVID, or a sinus infection, but dust, pollen, pollution, and other inhaled irritants also can trigger flares.
“If you have more severe COPD or your health is fragile, big changes in the weather also can cause a flare,” adds Dr. Beuther.
When a flare occurs, your airways swell more than usual. That narrows the passage that carries air through your lungs. More mucus also gets produced, and it may be thicker than normal. This further restricts your breathing. It also makes you cough and wheeze more, says Dr. Mina. Hyperinflation gets worse as you become less able to empty your lungs.
“The impact of hyperinflation on the respiratory muscles is more augmented at this point, so you get a worsening of your breathing pattern,” says Dr. Mina.